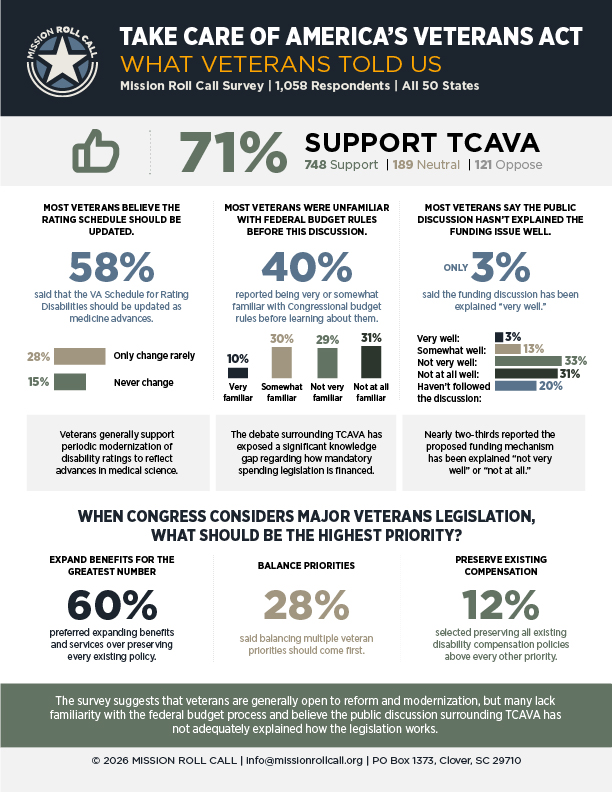
As Congress considers the Take Care of America’s Veterans Act (TCAVA), Mission Roll Call asked veterans what they believe should guide major veterans legislation. Rather than focusing on political rhetoric or competing advocacy campaigns, we wanted to hear directly from the people who rely on the Department of Veterans Affairs every day. The result is a snapshot of how veterans view the legislation’s priorities, the broader debate surrounding it, and the issues they believe deserve Congress’s attention.
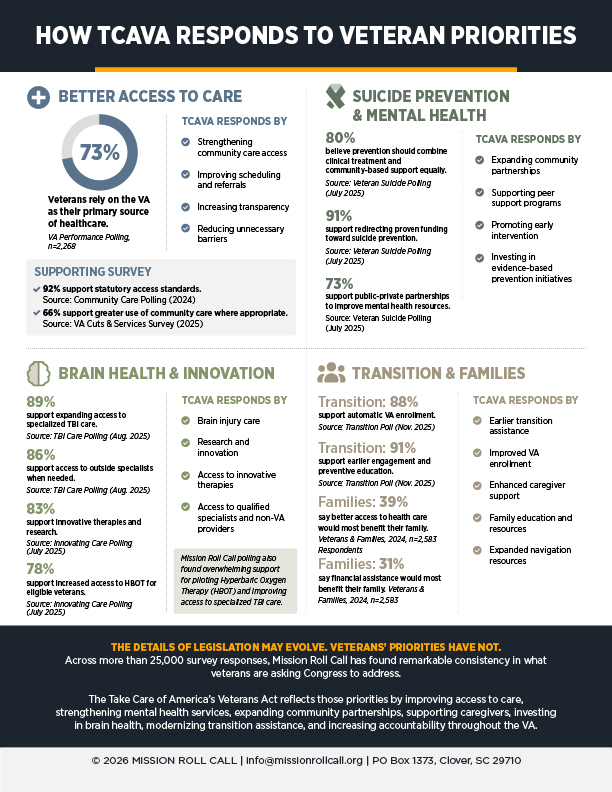
The findings presented here combine Mission Roll Call’s latest national survey of 1,058 veterans, as of July 13th, with results from more than 25,000 veteran, family member, and caregiver survey responses collected between 2024 and 2026. Across that research, veterans have consistently identified access to care, suicide prevention, brain health, caregiver support, transition assistance, innovation, and accountability as among the VA’s highest priorities. Those same priorities are reflected throughout the Take Care of America’s Veterans Act, providing an opportunity to compare the legislation with the issues veterans themselves have repeatedly said matter most.
Mission Roll Call does not conduct polling to tell veterans what to think. We do it to listen. We conduct research to ensure policymakers understand what veterans are saying. We hope the information in this report contributes to a more informed discussion and helps Congress, the media, and the public evaluate the legislation through the perspective of those it is intended to serve.
Clicking on any of the pages below will open the full report in a new browser tab.

Survey Methodology
Mission Roll Call’s mission is not to tell veterans what to think—it is to ensure policymakers know what veterans think.
About This Survey: Mission Roll Call conducts independent surveys to better understand the views, experiences, and priorities of America’s military and veteran community. The results help inform policymakers, veterans’ organizations, the media, and the public on issues affecting those who have served and their families.
This survey is open to individuals who identify as connected to the veteran community, including Veterans, Active Duty, National Guard, Reserve, Military Spouses, Family Members, Caregivers, and Survivors. Unless otherwise noted, published findings may report results for veterans specifically or for the broader military and veteran community, depending on the question being analyzed.
Participation is voluntary. Each participant is encouraged to complete the survey only once. Mission Roll Call employs technical safeguards and data quality reviews to identify duplicate or incomplete submissions before results are analyzed.
To strengthen confidence in the findings, Mission Roll Call may distribute the same survey through multiple recruitment channels, including its established participant network, public survey links, and partner organizations. Comparing results across these recruitment methods helps assess whether findings remain consistent regardless of how participants entered the survey.
Mission Roll Call is committed to transparency. Survey reports include field dates, sample size, methodology, and questionnaire details whenever practical. Results are reported regardless of whether they support or challenge Mission Roll Call’s policy positions.
FAQ
Who can participate?
Individuals who identify as Veterans, Active Duty, National Guard, Reserve, Military Spouses, Family Members or Caregivers, and Survivors.
How is my information used?
Survey responses are analyzed in aggregate and used to better understand the views of the military and veteran community. Individual responses are not publicly attributed.
Can I take the survey more than once?
No. Please complete each survey only once. Mission Roll Call uses quality-control procedures to identify duplicate submissions.
Are all survey results published?
Mission Roll Call publishes findings based on completed surveys and is committed to reporting results regardless of whether they support or challenge the organization’s policy positions.
How the Briley-Edmundson Act Seeks to Update Benefits for These Veterans
For veterans living with catastrophic service-connected injuries and for surviving spouses/children who lost a loved one because of military service, financial support is supposed to provide stability in the face of lifelong hardship. But while the nature and cost of care have changed dramatically over the past three decades, the foundational structure of many of these benefits has remained largely frozen in time. Congress is now debating whether that should finally change through the Briley-Edmundson Act (H.R. 6047), legislation aimed at increasing support for the nation’s most severely injured veterans and surviving families. The debate has forced lawmakers to wrestle with difficult questions surrounding fairness, priorities, and how expanded support should be funded within existing federal budget rules.

At the center of the legislation are Dependency and Indemnity Compensation (DIC) benefits for surviving spouses and Special Monthly Compensation (SMC) benefits for veterans with catastrophic injuries requiring daily care. These are not convenience benefits or occasional forms of assistance. They are critical support systems for veterans who often depend on full time caregiving, specialized medical equipment, rehabilitation services, housing modifications, and long-term care simply to remain outside institutional settings. Yet despite the intensity of those needs, many of the underlying benefit structures have not seen meaningful base rate changes since the late 1980s and early 1990s. While annual cost of living increases have occurred, those adjustments have generally followed ordinary inflation rather than the much steeper rise in medical and caregiving costs. Over time, the gap has become impossible for many families to ignore.
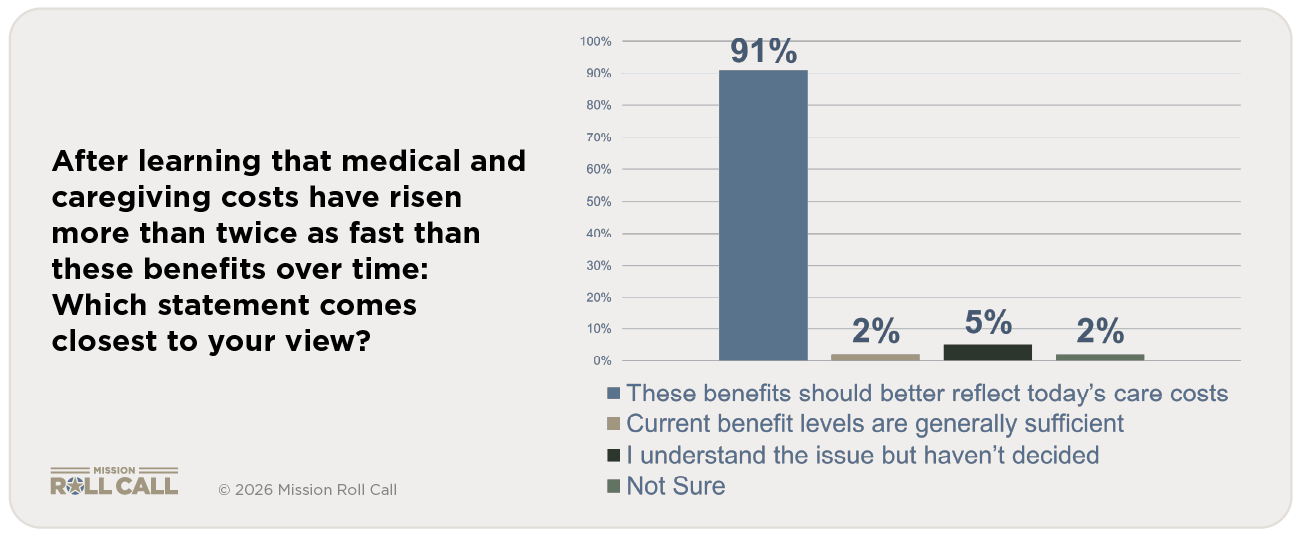
Mission Roll Call’s recent national survey on the Briley-Edmundson Act found overwhelming support among veterans, caregivers, and military families for revisiting these outdated benefit structures. More than 845 respondents participated in the survey, which examined support for expanding DIC and SMC benefits as well as broader attitudes surrounding funding tradeoffs and fiscal responsibility. After learning that medical and caregiving costs have risen more than twice as fast as these benefits over time, ninety one percent of respondents said benefits should better reflect today’s care costs. One veteran participating in the survey summarized the frustration simply: “These families are dealing with costs that didn’t even exist when these rates were first created. The system has not kept up with reality.”
The survey also revealed broad agreement that Congress has a responsibility to revisit older benefit structures when economic realities fundamentally change. Eighty-eight percent of respondents agreed it is reasonable to reevaluate benefits that were established decades ago and adjusted primarily through inflation increases alone. Respondents also consistently identified support for severely injured veterans and surviving families as one of the most important priorities within the broader veteran support system. For many families, the issue is not theoretical. Caregivers often spend years or decades providing around the clock support while sacrificing careers, retirement savings, and long-term financial stability in the process. After the veteran passes away, surviving spouses can face an abrupt financial cliff despite years spent serving as unpaid caregivers inside the home. As one surviving spouse explained, “When my husband passed, the caregiving stopped but the financial pressure didn’t. The bills and responsibilities were still there, but the support system suddenly changed overnight.”

The broader veteran community is increasingly unified on the issue. In a joint letter to House Veterans’ Affairs Committee leadership, organizations including Paralyzed Veterans of America, Wounded Warrior Project, Disabled American Veterans, AMVETS, and the Elizabeth Dole Foundation argued that updating these programs is “long overdue.” The groups emphasized that Special Monthly Compensation provides veterans with profound service-connected disabilities the financial ability to maintain some level of independence and quality of life, while Dependency and Indemnity Compensation protect surviving spouses from financial instability after the loss of a veteran.
Importantly, veterans responding to the survey also acknowledged the complexity of balancing competing priorities across the VA system. Many respondents supported balancing expanded catastrophic injury benefits with preserving broader programs like the VA Home Loan program. But even amid those tradeoffs, the central message remained remarkably consistent: veterans and families carrying the heaviest burdens should not continue falling behind because support systems failed to evolve alongside modern medical and caregiving realities. As another respondent stated, “No one is asking for luxury. They’re asking for benefits to reflect what caregiving and survival actually cost in 2026.”
The wars of the last twenty years produced a generation of veterans surviving injuries that would not have been survivable in earlier conflicts. Advances in battlefield medicine saved lives, but many of those survivors now require decades of intensive and expensive care. For many veterans, the Briley-Edmundson Act ultimately comes down to a question of fairness. The nation asked these veterans and families to carry extraordinary burdens in service to the country. Expecting financial support systems built around economic assumptions from the late 1980s and early 1990s to fully sustain those burdens today is becoming increasingly difficult to justify. As Congress debates the legislation in the coming weeks, veterans are sending a clear message: support for the nation’s most severely injured veterans and surviving families should reflect the realities of modern caregiving, modern medical costs, and modern life.
Mission Roll Call’s February 2026 survey of more than 2,200 veterans asked respondents to gauge the VA’s change in performance one year after Secretary Collins was appointed. The results point to a Department of Veterans Affairs that is holding steady, with modest signs of improvement over the past year. But stability, particularly in a system serving a growing and evolving veteran population, is not the same as progress.
The key question we asked in this survey was:
Thinking about your experiences with the Department of Veterans Affairs over the past year, please indicate whether each area has gotten better, stayed about the same, or gotten worse.
View the Full Report
Overall VA Performance

Nearly half of respondents say overall VA performance has stayed about the same, while 38% report improvement and 17% report that conditions have worsened. This distribution suggests that while positive movement is occurring, it has not yet translated into a consistent experience for most veterans.
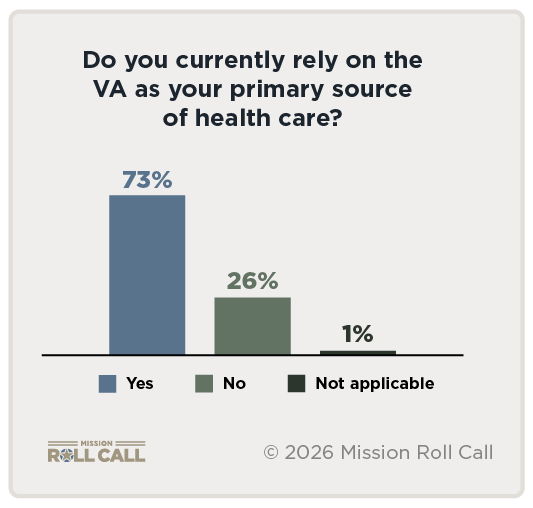
That distinction matters. Seventy-three percent of respondents rely on the VA as their primary source of health care, meaning that incremental gains are often overshadowed by day-to-day realities around access, timeliness, and continuity of care. For these veterans, performance is measured in whether they can get an appointment when they need one, maintain a relationship with a provider, and receive care without unnecessary delay.
The data reflects a system that is trending in the right direction but not yet keeping pace with demand. Improvements in overall performance and quality of care are evident but often constrained by underlying challenges in staffing and access.
Access to Care Remains the Defining Issue
Demand for VA services remains high, and for many veterans, the system is a central part of their health care. Survey responses show widespread use across primary care, specialty care, and community care, reinforcing how heavily veterans rely on the VA to meet both routine and complex medical needs.
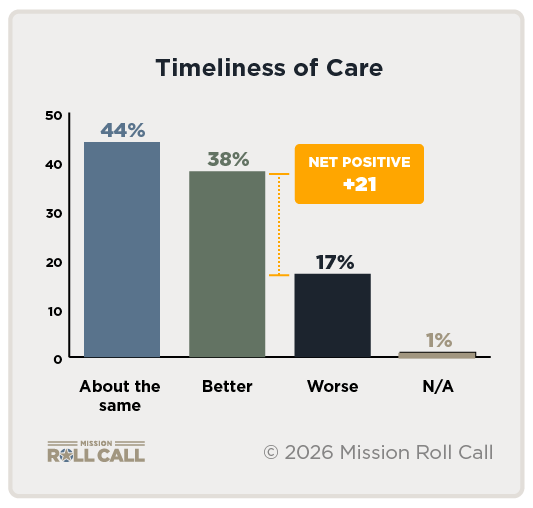 Across multiple categories, veterans report a similar pattern: the system works, but not always when they need it. As shown in the graphic, Timeliness of Care mirrors overall performance, with 44% of respondents saying it has stayed the same, 38% reporting improvement, and 17% reporting it has worsened. These numbers suggest that while progress is being made, it has not yet translated into a reliably faster or more responsive experience for most veterans.
Across multiple categories, veterans report a similar pattern: the system works, but not always when they need it. As shown in the graphic, Timeliness of Care mirrors overall performance, with 44% of respondents saying it has stayed the same, 38% reporting improvement, and 17% reporting it has worsened. These numbers suggest that while progress is being made, it has not yet translated into a reliably faster or more responsive experience for most veterans.
This gap between availability and accessibility shows up in practical ways. Veterans often describe delays in scheduling, long wait times for specialty care, and difficulty navigating referrals—particularly when transitioning between VA providers and community care. For those living in rural areas or managing ongoing conditions, these delays turn routine care into a prolonged process.
 Community care has expanded options for many veterans, but it has also introduced additional complexity. While some report positive experiences, others point to delays in authorization, lack of coordination between providers, and confusion about eligibility or next steps. The VA system offers more pathways to care, but not always a clearer or faster route to receiving it.
Community care has expanded options for many veterans, but it has also introduced additional complexity. While some report positive experiences, others point to delays in authorization, lack of coordination between providers, and confusion about eligibility or next steps. The VA system offers more pathways to care, but not always a clearer or faster route to receiving it.
Staffing Shortages Continue to Limit Access
Behind many of the access challenges veterans report is a more fundamental constraint: staffing.
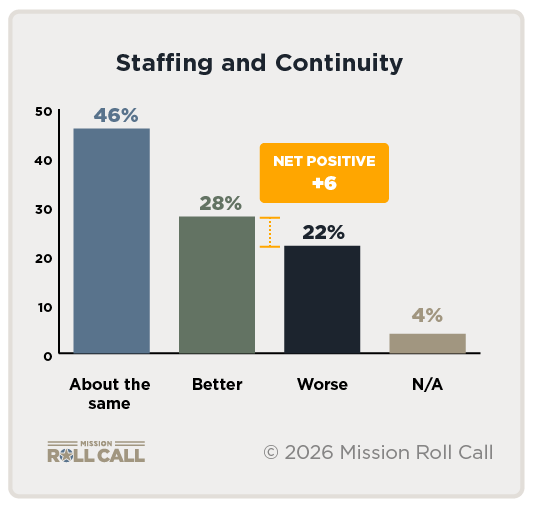 Survey results show that staffing and continuity of care remain among the weakest performing areas. Nearly half of respondents say conditions have stayed the same, while a higher percentage of veterans report worsening conditions, producing one of the lowest scores across all categories.
Survey results show that staffing and continuity of care remain among the weakest performing areas. Nearly half of respondents say conditions have stayed the same, while a higher percentage of veterans report worsening conditions, producing one of the lowest scores across all categories.
When staffing levels are insufficient, the effects show up in different ways. Appointment availability declines and wait times increase. Veterans are more likely to see different providers from one visit to the next, making it harder to build continuity and trust.
The takeaway from the data shows that access and timeliness cannot be achieved without addressing staffing capacity. Scheduling systems and referral pathways can be refined, but without enough providers to meet demand, those improvements will have limited impact.
Mental Health Access Remains Inconsistent
 Mental health care is one of the most critical services the VA provides, and it is where the system’s strengths and limitations are most clearly felt.
Mental health care is one of the most critical services the VA provides, and it is where the system’s strengths and limitations are most clearly felt.
Survey results show that access to mental health care has made incremental improvement, but remains uneven. While some veterans report improvement, a significant portion indicate no change. Taken together, these responses point to a system that is not consistently reaching all veterans who may need support.
Unlike other areas of care, gaps in mental health services can have more immediate and lasting consequences.
Veterans frequently describe difficulty maintaining consistent relationships with providers, particularly when staffing shortages lead to turnover or reassignment. In a field where trust and continuity are essential, disruptions in care can make it harder to sustain progress or seek help during periods of need.
These figures suggest the VA should keep a close eye on the relationship between staffing and mental health care. When mental health professionals are in short supply, appointment availability declines and wait times increase. This can lead to delayed care, reduced session frequency, and greater reliance on already stretched providers.
Stability Is Not Enough
The VA is showing improvement in the first year of Secretary Collins’ tenure, though work remains.
Over the past year, the department has made targeted investments in the right areas. Efforts to improve scheduling and referral systems, strengthen continuity of care, and modernize how care is delivered are beginning to show up in performance data. Veterans are reporting gains in overall performance and quality of care, and the VA has taken steps to improve how it coordinates with community providers and processes payments. These are meaningful moves, and they reflect a system that is focused on the right problems.
Progress leads to performance at scale, and there are notable areas for continued improvement. The most consistent constraint remains staffing. Without enough providers, improvements to scheduling, referrals, and community care cannot deliver the access veterans need. The result is what veterans are reporting: a system that is getting better in places, but still inconsistent when it matters.
Veterans are not disengaged from the political process. If anything, they are among the most consistent participants in it. But political leadership is not building confidence within the veteran voting bloc.
Mission Roll Call’s March 2026 survey of more than 1,600 respondents shows a veteran community that is paying attention, showing up, and voting—but increasingly questioning whether their priorities are reflected in the decisions that follow.
A Highly Engaged Electorate
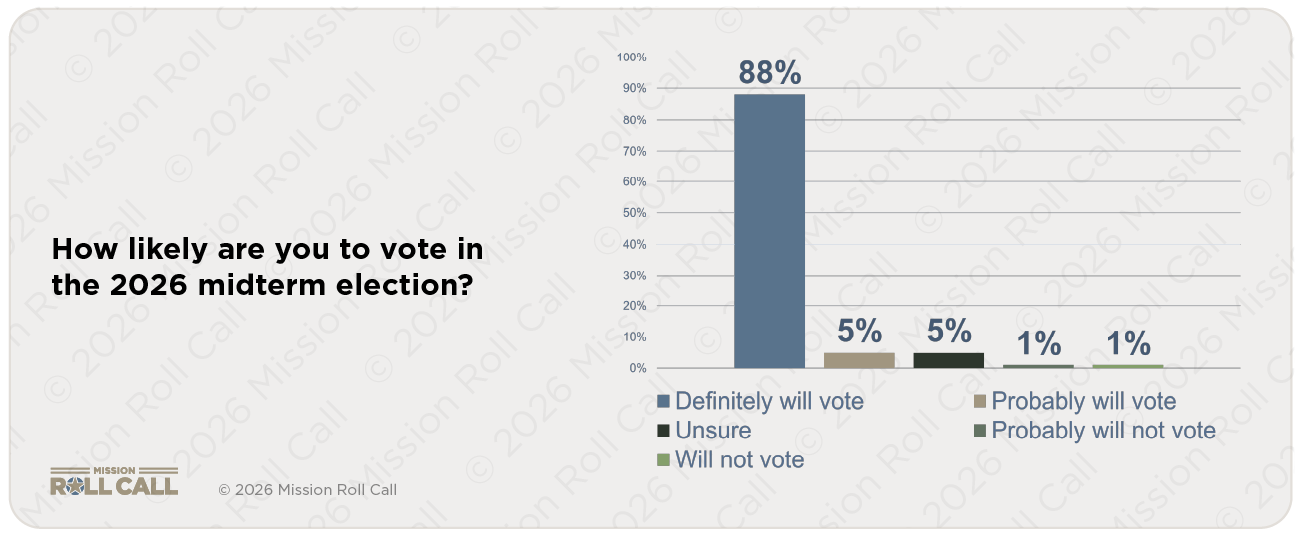
Veterans are not disengaged from the political process. In fact, they are among the most reliable and committed voting blocs in the country. According to the survey, nearly 90 percent of respondents say they will definitely vote in the 2026 midterm elections, with only a small percentage indicating uncertainty or a likelihood of sitting out. This level of participation is not incidental. It reflects a population that continues to see civic engagement as an extension of service and responsibility, even years after leaving the military.
At the same time, engagement does not equal satisfaction. What emerges clearly from the data is a growing frustration with how veteran issues are handled once the election cycle ends. As one respondent put it bluntly, “Communication, veterans’ rights are not being enforced.” That sentiment underscores a broader concern: veterans are participating, but they are not convinced they are being heard or taken seriously in the decisions that follow.
Top Issues: Personal Stakes, National Consequences
When asked what issues will most influence their vote, veterans pointed to a mix of deeply personal concerns and broader national priorities. Disability compensation and benefits ranked highest, followed closely by economic conditions and inflation, while national security and military readiness remain central. These priorities reflect the dual perspective veterans bring to public policy, balancing both personal stability and the broader direction of the country.
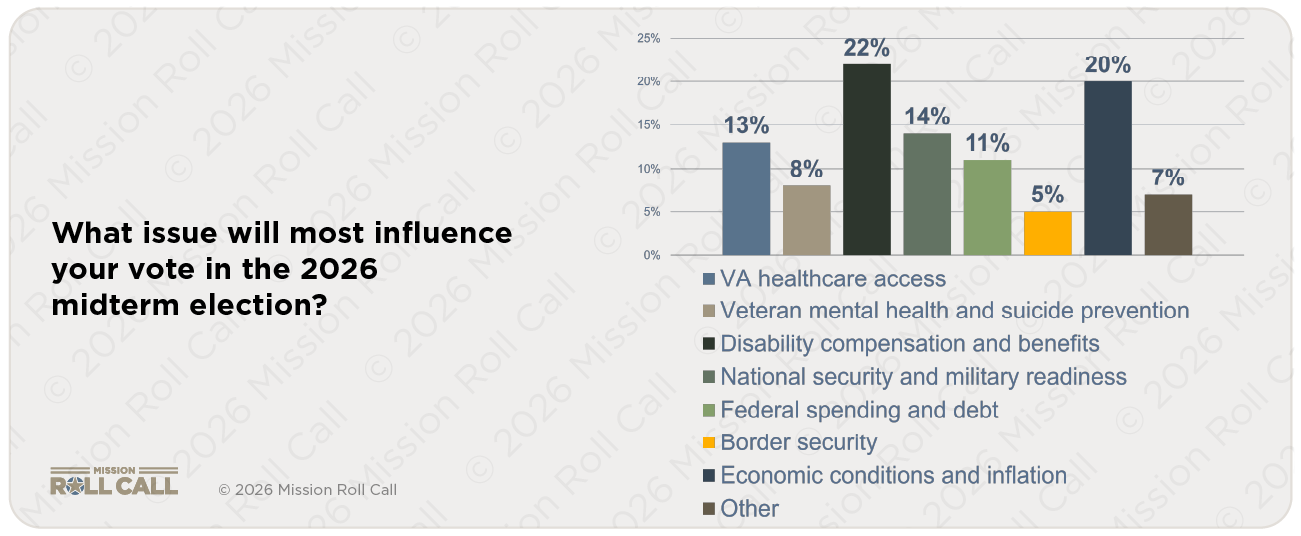
The connection between these issues is clear in the responses themselves. One veteran pointed to “inflation, decreased healthcare coverage for veterans, and the overall quality of care” as interconnected concerns, reinforcing how economic pressure and access to benefits often overlap in daily life. Healthcare access, particularly within the VA, continues to play a major role, though it falls slightly behind financial and compensation related issues, suggesting that immediate economic pressures are shaping how veterans prioritize their concerns.
At the same time, mental health remains a persistent and underlying issue. While it ranked lower as a direct voting driver, open ended responses tell a more urgent story, with veterans pointing to “PTSD issues” and warning that “mental health care will still fall short.” This gap between ranking and lived concern suggests that mental health is not secondary, but embedded within broader challenges of access, stability, and long term care.
Clear and Consistent Priorities for Congress
When asked what Congress should prioritize, protecting VA funding emerged as the top priority by a wide margin, followed by ending veteran homelessness and expanding access to community care.

Veterans reinforced these priorities in their own words, adding depth to the data. “Ending veteran homelessness,” one respondent wrote simply, while another emphasized the importance of “proper staffing of existing VA facilities,” highlighting operational gaps that directly impact access and quality. Others focused on how care is delivered, including the “need for more care options outside the VA healthcare system” and the importance of improving navigation and usability.
As one veteran explained, meaningful reform includes “streamlining and making it easier for technology-challenged veterans to get their care and benefits.” Taken together, these responses point to a need for execution, consistency, and follow through on commitments that already exist.
A Confidence Gap That Continues to Widen
Despite strong engagement and clearly defined priorities, confidence in Congress remains limited, revealing a widening gap between participation and trust. A majority of respondents reported low or no confidence that lawmakers will protect VA healthcare funding over the next two years. This lack of confidence extends beyond funding decisions and into the broader political environment, where more than two thirds of respondents believe veteran issues do not receive adequate attention from candidates during election cycles. Even more striking, an overwhelming majority agreed that veterans are often used as political talking points without meaningful follow through.
Veterans are not questioning whether they are mentioned in speeches. They are questioning whether those mentions lead to action. That concern becomes even more pronounced when looking at long term care needs, with one respondent emphasizing the importance of supporting “disabled veterans and those with PTSD when they are no longer able to advocate for themselves.” This reflects a deeper issue of responsibility and trust that cannot be addressed through messaging alone.
Strengthening the System, Not Replacing It
When it comes to healthcare delivery, veterans are asking for a system that works more reliably. The most widely supported approach is a balance between VA care and community care, rather than expanding one at the expense of the other. This reflects a pragmatic understanding of both the strengths and limitations of the current system.
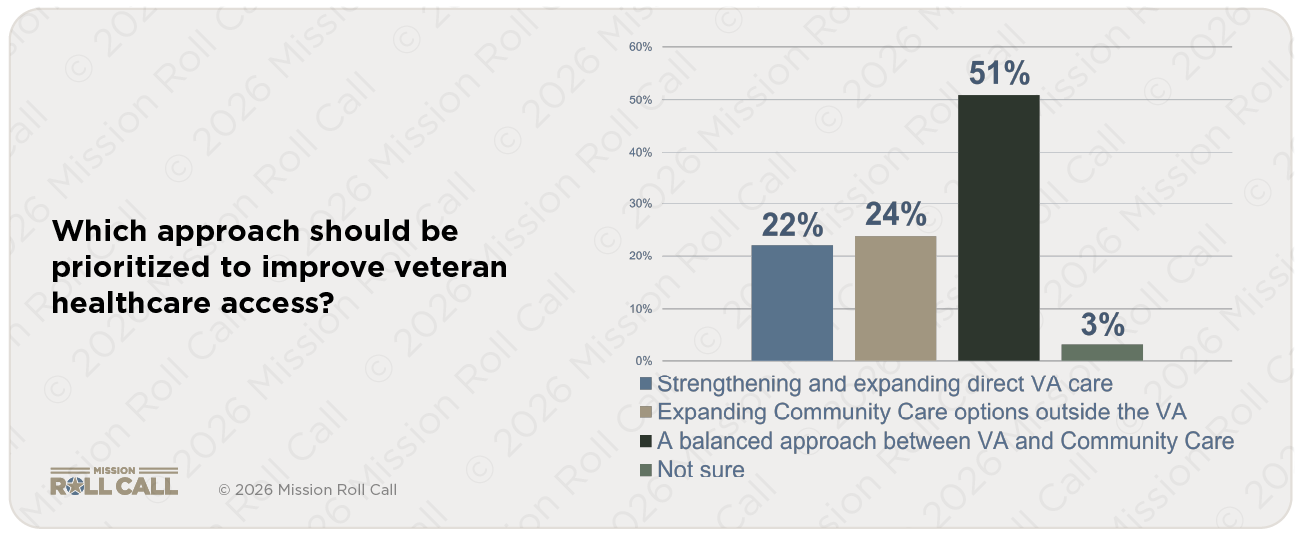
Satisfaction levels reinforce this complexity. Many respondents report being somewhat satisfied, while a significant portion report dissatisfaction. This middle ground points to a system that is functional but inconsistent, capable of delivering care but not always in a way that veterans can depend on. The message here is that the system isn’t working reliably enough to meet expectations across the board.
What Veterans Want From Leadership
Veterans were also clear about what would increase their trust and engagement in political leadership moving forward. Their responses point to a desire for clarity and accountability rather than additional outreach or messaging. Clear positions from candidates on veteran issues ranked highest, followed closely by transparency in VA funding decisions.
Notably, a significant number of respondents indicated that nothing would increase their likelihood of voting, reinforcing that this is not a population that needs to be mobilized. Veterans are already engaged. The question is whether their engagement is being met with meaningful action and responsiveness from those in positions of leadership.
The Bottom Line
These survey results ultimately paint a picture of a population that remains committed to civic participation while growing increasingly frustrated with the outcomes that follow. Veterans are engaged, informed, and paying attention not just to what is said, but to what is done. They are asking for follow through, for accountability, and for systems that function consistently rather than intermittently. Above all, they are asking to be heard, not just during election cycles, but in the policies that shape their daily lives. For lawmakers, the message is straightforward: veterans are watching, and they are voting.
As the 2026 midterm election approaches, decisions made in Washington will shape the future of veterans’ healthcare, benefits, and support systems for years to come. Those decisions should be informed by the voices of veterans themselves.
As we do every month, Mission Roll Call is launching a national survey on March 1st to ensure that veterans help define the priorities and expectations that will guide the next Congress and the future direction of the Department of Veterans Affairs.
The issues facing veterans are daily realities, but they are often lost in the abstract policy debates so often witnessed in Washington. As we know, elections have consequences, and the 2026 mid-term is no different. Elected leaders will continue to debate important issues impacting veterans. Access to timely, high-quality care. Mental health and suicide prevention. Disability compensation and long-term sustainability of the system. The balance between direct VA care and community-based options. These are structural questions that will be shaped by the outcomes of the 2026 election and the leadership that follows.
This survey is designed to do more than measure opinion. It will identify what issues veterans believe should define the national conversation, how much confidence they have in Congress to protect VA funding, and what expectations they have for candidates seeking federal office. It will also examine how veterans view civic engagement itself—whether elected officials are providing adequate attention to veteran issues and whether greater accountability is needed.
Veterans understand service and responsibility. This survey recognizes that civic engagement does not end when military service concludes. It continues in how veterans vote, how they participate, and how they hold institutions accountable.
The results of this survey will be shared directly with congressional offices, VA leadership, policymakers across the country, and of course you – the veteran. They will help shape advocacy efforts and ensure that legislative priorities reflect documented veteran perspectives—not assumptions.
The strength of this effort depends on participation. The more veterans who engage, the clearer and more influential the message becomes.
In 2026, your voice should help shape the path forward.
Traumatic brain injury (TBI) remains one of the most common and complex injuries affecting post-9/11 veterans. While awareness and diagnosis have improved over the past two decades, many veterans continue to face limited treatment options, long wait times, and care models that do not fully address the long-term cognitive, emotional, and social effects of brain injury. New bipartisan legislation introduced in Congress aims to change that.
![]()
The BEACON Act, introduced by Jack Bergman (R-MI) and Sarah Elfreth (D-MD), seeks to modernize how the Department of Veterans Affairs delivers care to veterans with mild to moderate TBI. The bill focuses on expanding access to evidence-based, non-pharmacological therapies and strengthening partnerships between the VA and leading civilian, academic, and nonprofit institutions.
For many veterans, TBI does not exist in isolation. It often intersects with post-traumatic stress, sleep disorders, depression, chronic pain, and difficulties reintegrating into civilian life. Current treatment pathways can be fragmented or overly reliant on medication, leaving veterans and families searching for alternatives that better address the full scope of their needs. The BEACON Act is designed to help close these gaps by supporting innovation and accelerating the integration of proven therapies into VA care.
![]()
The legislation would establish two new VA grant programs. One would support clinical research, provider training, veteran and family outreach, and partnerships focused on effective non-pharmacological treatments. The second would advance independent research and implementation of validated therapies, with oversight modeled after the VA’s National Center for PTSD. Together, these programs aim to move promising treatments from research settings into consistent, real-world clinical use.
The bill’s emphasis on outcomes is particularly significant. By prioritizing cognitive function, mental health, and quality of life, the BEACON Act recognizes that successful TBI care must extend beyond symptom management. Improving access to comprehensive, evidence-based treatment can play a meaningful role in reducing long-term disability, improving employment and family stability, and lowering suicide risk among affected veterans.
![]()
Support for the BEACON Act reflects broad agreement across the veteran community that current systems need to evolve. National organizations such as American Legion (https://www.legion.org) and Avalon Action Alliance (https://www.avalonactionalliance.org) have endorsed the legislation, underscoring shared recognition that innovative, whole-person approaches to brain health are long overdue.
Mission Roll Call supports bipartisan efforts to improve care and outcomes for veterans living with traumatic brain injury. The BEACON Act represents an important step toward a more modern, flexible, and veteran-centered approach—one that reflects what veterans consistently report they need most: access to effective care that works in practice, not just in theory.
As Congress considers this legislation, Mission Roll Call will continue engaging with policymakers to ensure veteran voices remain central to the discussion and that reform efforts translate into meaningful, measurable improvements in care.
Mission Roll Call launched 2026 with a bipartisan kickoff reception on Capitol Hill, bringing together senior federal leaders, policymakers, veteran advocates, and partners from across the veteran and military community. The event underscored Mission Roll Call’s commitment to elevating veteran voices and advancing practical, veteran-driven policy solutions.

The reception featured remarks from Secretary of Veterans Affairs Doug Collins, House Committee on Veterans’ Affairs (HVAC) Chairman Mike Bost (IL), and House Appropriations Committee Ranking Member Debbie Wasserman Schultz (FL). Also in attendance was HVAC Subcommittee on Health Chairwoman Mariannette Miller-Meeks (IA), HVAC Member General Jack Bergman (MI), and HVAC Member Tom Barrett (MI). Their participation highlighted the continued bipartisan focus on veterans’ health care, benefits, and long-term well-being at a critical moment for federal veterans’ policy.
Mission Roll Call CEO Jim Whaley hosted the evening, welcoming attendees and emphasizing the organization’s mission to ensure veterans’ experiences inform decision-making in Washington. Strategic Director of Government Affairs and Advocacy Mike Desmond served as emcee, guiding the program and reinforcing the importance of collaboration between Congress, the Department of Veterans Affairs, and the broader veteran community.

Speakers addressed the evolving needs of veterans following two decades of sustained conflict, including access to timely and effective health care, mental health and brain injury treatment, accountability within federal systems, and the challenges veterans and military families face during transition to civilian life. Throughout the program, speakers emphasized that durable solutions require both strong oversight and consistent engagement with veterans themselves.


The event drew participation from across the veteran community, including representatives from veteran service organizations, military family advocates, health care innovators, congressional staff, and nonprofit leaders. Conversations throughout the evening reflected shared priorities for the year ahead and reinforced the value of cross-sector coordination in driving meaningful progress for veterans and their families.
Mission Roll Call’s 2026 Kickoff Reception highlighted the organization’s role as a bridge between veterans and policymakers. Through national polling, veteran outreach, and direct engagement with policymakers, Mission Roll Call continues to translate veteran perspectives into actionable policy recommendations. The reception demonstrated that work in action, creating space for dialogue, relationship-building, and alignment across ideological and institutional lines.

Photos from the event and links to the speakers’ remarks are included below. Mission Roll Call thanks all who joined the reception and contributed to a strong start to 2026. The organization remains focused on advancing bipartisan, results-oriented policies that reflect the real priorities of veterans and military families nationwide.

On January 13, 2026, Mission Roll Call’s Chief Executive Officer, Jim Whaley, testified before the House Committee on Veterans’ Affairs Subcommittee on Health in Washington, D.C., to present the veteran community’s data-driven priorities on a broad slate of legislation addressing critical areas of veteran health care. The hearing focused on policies related to suicide prevention, traumatic brain injury, access to care, mental health, addiction treatment, and innovations in care delivery.

Jim opened his remarks by reiterating Mission Roll Call’s mission: to bring unfiltered veteran perspectives directly into policymaking through systematic polling and engagement. He emphasized that the bills under consideration — from the RECOVER Act to the BEACON Act, as well as proposals on access, TBI care, and pain management — reflect problems veterans have consistently identified in MISSION ROLL CALL’s national surveys.
Bringing the Veteran Voice to Suicide Prevention
Jim highlighted data from Mission Roll Call’s National Suicide Prevention Survey (July 2025) showing that veterans see suicide prevention not as a single program issue but as a system problem requiring multiple tools. A large majority of respondents emphasized that suicide prevention requires both clinical treatment and community-based support working together, and that community providers must be included in prevention efforts. Veterans also stressed the importance of training, coordination, and accountability in suicide prevention strategies.
In his testimony, Jim noted that the RECOVER Act (H.R. 2283) aligns with these priorities by expanding community-based mental health capacity, supporting provider training on veteran risk factors, and requiring transparent outcome reporting so policymakers and health systems can evaluate what works in practice.
Addressing Gaps in Traumatic Brain Injury Care
Jim also discussed the significant access challenges veterans face in obtaining appropriate care for traumatic brain injury (TBI). Drawing on MISSION ROLL CALL’s TBI Priorities Survey (August 2026), he noted that an overwhelming majority of veterans believe access to specialized TBI care is extremely important, yet many who seek care find it difficult to obtain.
He highlighted the BEACON Act as responding directly to that need by establishing a structured, evidence-based framework for evaluating innovative neurorehabilitation approaches — including rigorous independent outcome measurement and clear criteria for expanding access based on real results.

Modernizing Care and Accountability
In addition to TBI and mental health, Jim voiced support for measures that modernize how the VA delivers care. He testified in favor of the NOPAIN for Veterans Act and Veterans Mental Health and Addiction Therapy Quality of Care Act (H.R. 2426), describing how MISSION ROLL CALL’s broader polling shows veterans are concerned about overly narrow treatment approaches, want evidence-based options, and value care that can be evaluated and improved over time.
These bills — when considered together — reflect priorities veterans have repeatedly expressed: the need for expanded, measurable options that reduce risk and improve outcomes across the health care system.
Improving Access in Rural and Remote Communities
Another theme of Jim’s testimony was the persistent access gaps in rural, remote, and overseas communities. Citing data from Mission Roll Call’sACCESS Act Survey, he underscored veteran support for expanding community care options, streamlining access processes, and ensuring care is available when and where it is needed.
Jim expressed support for the Veterans Health Desert Reform Act and the U.S. Vets of the Freely Associated States Act as vehicles to leverage community providers, telehealth, and pharmacy services to break down geographic barriers to care.
A Data-Driven Path Forward
Throughout his testimony, Jim stressed that good policy starts with listening and that veterans consistently want transparent rules, reliable access, and accountability for outcomes. He concluded by urging Congress to continue grounding veteran health policy in the perspectives and experiences of those who have served.
A full video of the hearing and Jim Whaley’s complete testimony are available here and through the House Veterans’ Affairs Committee repository.
Inadequate family inclusion and support
Families and loved ones are often the first to recognize when a veteran begins to struggle physically, mentally, or emotionally, and their early awareness can make a world of difference for a veteran. Long before a challenge becomes a crisis, it is the spouse who notices the sudden withdrawal, the parent who hears something different in a phone call, or the sibling who sees a shift in routine. Yet during one of the most important periods in a veteran’s life, the transition out of the military, these same loved ones are often left on the sidelines. Because the separation process is fast paced, stressful, and packed with dense information, many veterans walk away without fully understanding the benefits they have earned or how to access them.
In our recent survey, 87 percent of respondents said they did not receive any follow-up from the VA or DoD after their separation. A percentage this high, combined with the veteran frustration outlined above, makes clear that a family member or trusted loved one should be involved in the discharge process. Families usually notice subtle changes in a veteran’s well-being long before a crisis occurs. If trusted family members also understand the benefits, enrollment steps, and programs available, they can help ensure nothing is missed.

Strategies Moving Forward
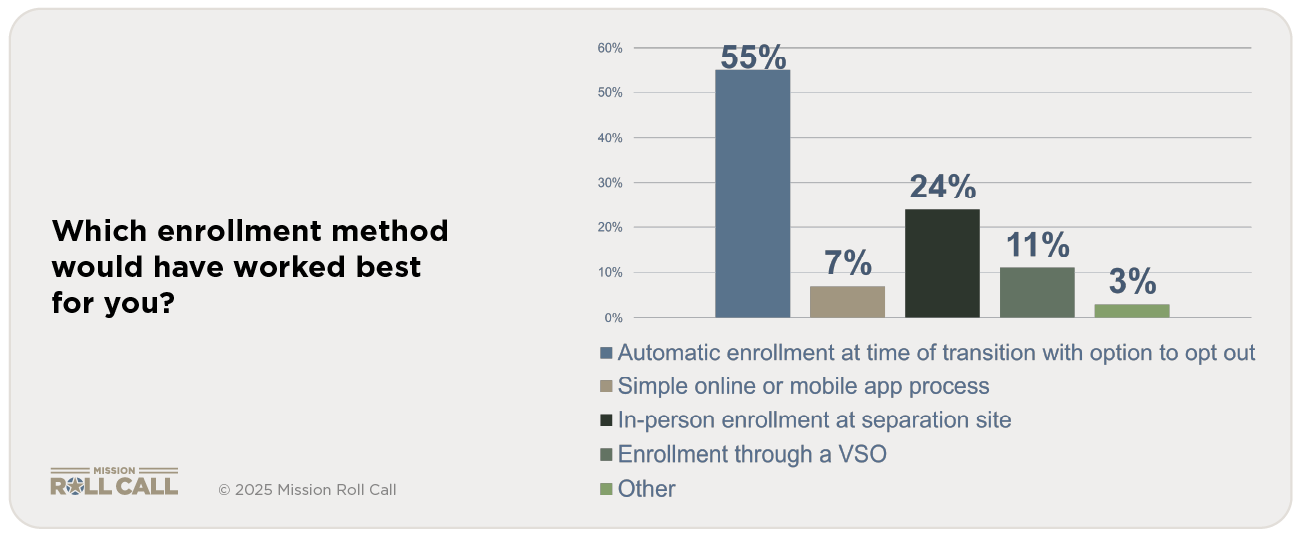
Recommendation #1: Automatic enrollment in VA at time of separation, with an option to opt out.
We asked veterans and their family members how they would prefer to be enrolled in the VA, and one answer stood out: automatic enrollment at the time of transition*, with the option to opt out. One way to ensure that all eligible servicemembers have access to the care provided by the VA is to automatically enroll them at the time of first eligibility, which is the moment they are separated from active duty with any discharge other than dishonorable.
*Some VA-related programs can be used before separation, such as the VA Home Loan Certificate of Eligibility, the Transition Assistance Program, and Pre-Discharge Disability Claims.
This option will guarantee that veterans have coverage and will make the transition easier. If a veteran does not want to take advantage of VA benefits, they will be able to easily opt out of coverage if they choose to do so.
Recommendation #2: Involve immediate family members or caregivers at critical moments during transition
Ensuring a family member or trusted advocate is present during VA enrollment and TAP instruction helps solidify understanding, spreads the burden of information retention, reduces the mental overload on the veteran, recruits the veteran’s own support network, and increases follow-through. A recent Mission Roll Call survey indicated that 69 percent of 595 family members/caregivers felt they were excluded in servicemember’s transition planning or enrollment discussion. Providing clearer, streamlined information that is delivered to servicemembers and their families can reduce confusion that occurs during an already stressful time.

Sharing information about VA programs, caregiver resources, and support services helps families prepare and advocate effectively. When families understand VA services before they are needed, veterans are more likely to connect with care early and maintain long-term engagement, reducing the burden on the veteran and their families.

This lack of clarity is compounded by the fact that many veterans were unsure whether they were ever clearly offered the opportunity to enroll in VA health care or benefits during transition.
![]()
This gap in communication and understanding leaves veterans, and especially younger veterans, navigating complex systems such as health care, education benefits, and disability compensation without the guidance or confidence needed to access what they have earned.
Moving Forward
Despite the programs and resources designed to support transitioning service members, many veterans leave the military feeling unprepared for civilian life. They encounter complex and confusing VA enrollment processes, often struggle to understand official guidance, and experience limited support from their families due to gaps in inclusion and communication. These challenges are particularly acute for younger veterans, who may enter service with little civilian experience, no professional networks, and few of the life skills necessary to navigate employment, healthcare, and financial responsibilities. Without targeted support, these veterans are at greater risk of underemployment, financial strain, housing instability, and mental health challenges, including depression and suicidal ideation.
Addressing these gaps requires a multi-pronged approach. Targeted transition support and mentorship can help veterans translate military skills into civilian credentials and career pathways. Clear, consistent communication from the Department of Defense and the VA, coupled with streamlined enrollment processes, can reduce confusion and delays in accessing benefits. Actively involving families in transition planning ensures that veterans have a support network that understands available resources and can intervene early when challenges arise. By implementing these measures, we can not only ensure veterans access the benefits they have earned, but also help them build stable, healthy, and fulfilling post-service lives, strengthening both individual outcomes and the broader community that relies on their contributions.
Every year, more than 200,000 men and women transition from military service to civilian life. Although policymakers frequently emphasize the goal of a “seamless transition,” the lived experience of veterans suggests that this goal remains unmet. Their families and loved ones often absorb the resulting challenges, providing support where existing systems fall short.
In October 2025, Mission Roll Call conducted a nationwide survey examining the transition process. More than 1,500 veterans and family members participated, offering frank assessments of current programs and support structures. Their responses reveal consistent themes: veterans do not feel thoroughly prepared for civilian life; they lack clear guidance on navigating VA benefits, and the broader system does not sufficiently address the needs of their families.
Our survey identifies four key areas in which the transition process falls short, leaving veterans and their families insufficiently prepared for life after service:
- Limited preparedness for civilian life: Half of veterans’ report feeling unprepared for the challenges of civilian life.
- Complex and unclear VA enrollment: The process of enrolling in VA benefits is often opaque, inconsistent, and more complicated than other aspects of transition.
- Low trust in DOD and VA guidance: Veterans frequently place low trust in official sources, instead relying on peers for guidance on transition-related tasks.
- Inadequate family inclusion and support: Families are often under-informed and excluded from the transition process.
Veterans often feel unprepared for life after service, face confusing and inconsistent VA enrollment, lack confidence in official guidance, and experience limited support for their families. We must address these gaps to ensure veterans and their loved ones receive the guidance and support they need for a successful transition.
Preparation for Civilian Life
We asked veterans how well their military service prepared them for civilian employment, education, and community life. The responses show that half of all veterans felt insufficiently prepared for life after service.

One veteran wrote in our survey, “I was trained to do my job, not to navigate civilian life.” Another said, “I did not know how to translate my skills into something employers understood.”
These comments align with the data. Veterans arrive in civilian life with strong, marketable skills developed through military service but receive too little guidance on how to translate those skills into civilian credentials, language, and career pathways. The impact is not abstract. When veterans cannot clearly articulate their experience to employers, they are more likely to be underemployed or unemployed, even when jobs are available. That underemployment often leads to financial strain, loss of identity and purpose, and growing frustration with systems that promised a seamless transition but did not deliver.
Over time, these pressures compound. Difficulty securing stable, meaningful work is a well-documented risk factor for housing instability and homelessness, particularly for younger veterans and those leaving the service without a strong civilian network. Prolonged economic stress and a sense of failure or invisibility can also deepen mental health challenges, increasing the risk of depression, substance use, and suicide. In this way, inadequate skills translation is not just a workforce issue; it is a public health and public safety issue.
Because many of the most at-risk veterans entered service so young, many had little experience managing personal finances, navigating healthcare, or making major life decisions before joining. The military’s structured environment provides housing, healthcare, and a clear professional pathway. Once separated, veterans are suddenly responsible for decisions previously handled by their chain of command.
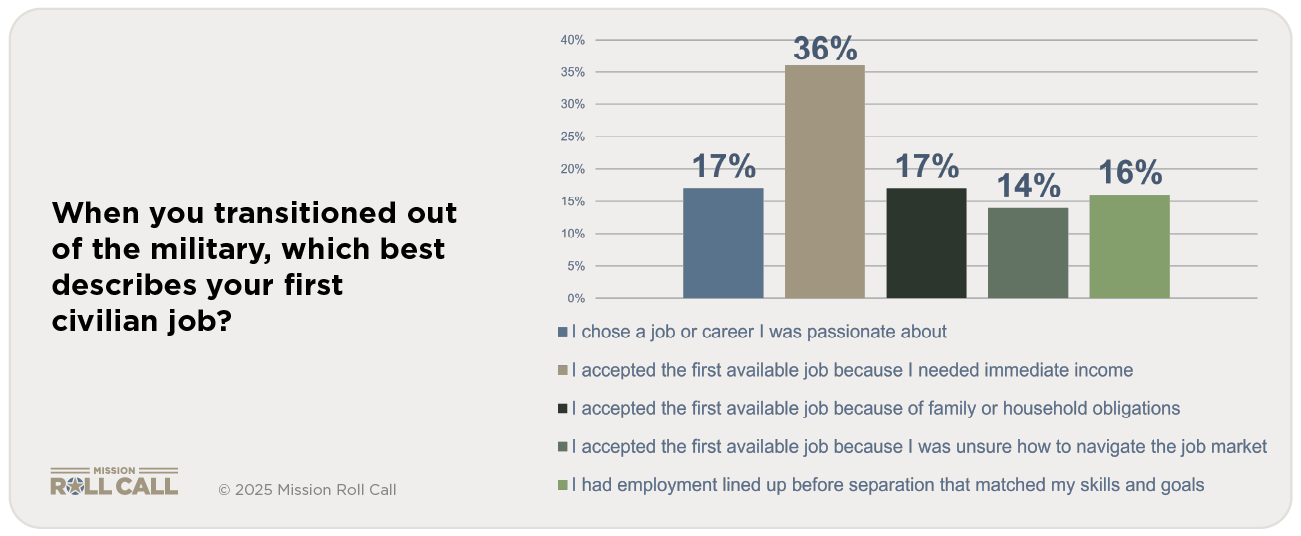
This pressure shows clearly in the job market. When asked which statement best describes their first civilian job, many respondents said they took the first job they could get. Perhaps more concerning, 67 percent of respondents did not choose a job based on fit, interest, or long-term career goals. They simply needed work or lacked guidance to make a more informed decision.
Unlike many older veterans who transition with more life experience, younger veterans often leave the military without strong community ties outside the service. The loss of camaraderie, routine, and purpose can create feelings of isolation or disorientation. These young service members often stepped into uniform at a time when their civilian peers were developing foundational life skills, pursuing education, and gaining early work experience.
As a result, many separate from the military without a college degree, without a professional network, and without the civilian work history employers expect. For some, the transition is not just a career shift but the end of the only adult life they have ever known. In the most serious cases, these pressures intersect with mental health challenges and increase risk for crisis or suicide.
These findings point to multiple areas of concern deserving of more focused solutions. Younger veterans require targeted and intensive support to successfully navigate the transition from military to civilian life. This includes:
- stronger communication about benefits
- more accessible and effective transition education
- financial guidance
- mentorship and career coaching
- community building and focused programs alongside veterans that replicates the cohesion they lose after separation
- By understanding where the gaps exist, we can ensure veterans enter civilian life with clarity, confidence, and connection instead of uncertainty and risk.
Complex and unclear VA enrollment
The process of enrolling in Department of Veterans Affairs benefits is often opaque, inconsistent, and more complicated than other aspects of the transition to civilian life. Compounding this challenge, our survey found that the Transition Assistance Program is frequently viewed as unhelpful or, in some cases, counterproductive. Even among veterans who did participate in TAP, only a small share reported that it meaningfully prepared them for what came next.

Veterans’ comments consistently point to problems with timing, delivery, and relevance. Many cited the speed at which information was presented, the lack of follow up, and content that felt disconnected from their immediate needs. One veteran described TAP as “information, not preparation.” Another noted that it “came at the end, when my attention was split between out processing tasks.”
Together, these responses reveal two critical gaps. First, a significant number of servicemembers never meaningfully engage with TAP at all. Second, for those who do, the program is often experienced as brief, generic, and easy to forget rather than as a sustained bridge to civilian life. These gaps leave veterans navigating complex benefit systems on their own at precisely the moment when clear guidance and continuity matter most.
Others described how the process competed with immediate financial and family pressures. “I was trying to find a job, move my family, and figure out health care all at once,” one veteran wrote. “VA enrollment just became another full-time job.”

For some veterans, the complexity and opacity of the VA enrollment process are so discouraging that they disengage entirely, particularly when faced with lengthy, repetitive, and confusing paperwork. Even minor errors can trigger significant delays, with forms often requiring repeated submissions across offices that do not communicate with one another. Veterans describe this experience as overwhelming, and as a result, some forego benefits entirely, delaying or losing access to healthcare, education programs, and financial support.
Low trust in DOD and VA guidance
Veterans consistently describe required forms as lengthy and difficult to understand, with unclear instructions and little support for completing them correctly. Many report being caught in cycles of submission and correction that erode confidence and momentum. One veteran stated, “After being sent in circles so many times, I just stopped trying.” Another explained, “I filled out the paperwork the best I could, only to be told months later that something was missing or wrong.”
Even small errors can trigger significant delays. As one respondent shared, “One mistake on a form meant everything was kicked back, and no one could tell me how to fix it.” Others described having to provide the same information repeatedly across different offices that do not communicate with one another. “I felt like I was doing the same paperwork over and over,” one veteran wrote, “but every time it was for a different system.”

These administrative barriers have real consequences. Delays in completing or correcting paperwork can postpone access to health care, education benefits, and income support for months or longer. Rather than serving as a stabilizing force during transition, unclear and burdensome paperwork often becomes an added source of stress and discouragement. For veterans already balancing employment, family responsibilities, and the emotional challenges of leaving military service, paperwork difficulties can be the tipping point that leads them to disengage entirely, leaving critical benefits unused.
At the same time, many veterans report low trust in official sources of transition information and instead rely on peers for guidance. Official briefings, websites, and help lines are frequently described as confusing, inconsistent, or disconnected from lived experience. One veteran explained, “I trusted other veterans more than anything I was told in a briefing.” Another shared, “The official information sounded good, but it did not match what actually happened once I got out.”
Peer networks are viewed as more credible because they offer practical, experience-based advice. Veterans commonly turn to friends who have already separated, informal online groups, or fellow servicemembers slightly ahead of them in the process. “I learned more from talking to other veterans than I did from any official program,” one respondent noted. Another added, “Other vets told me what paperwork actually mattered and what mistakes to avoid. That was never clear from the VA or TAP.”
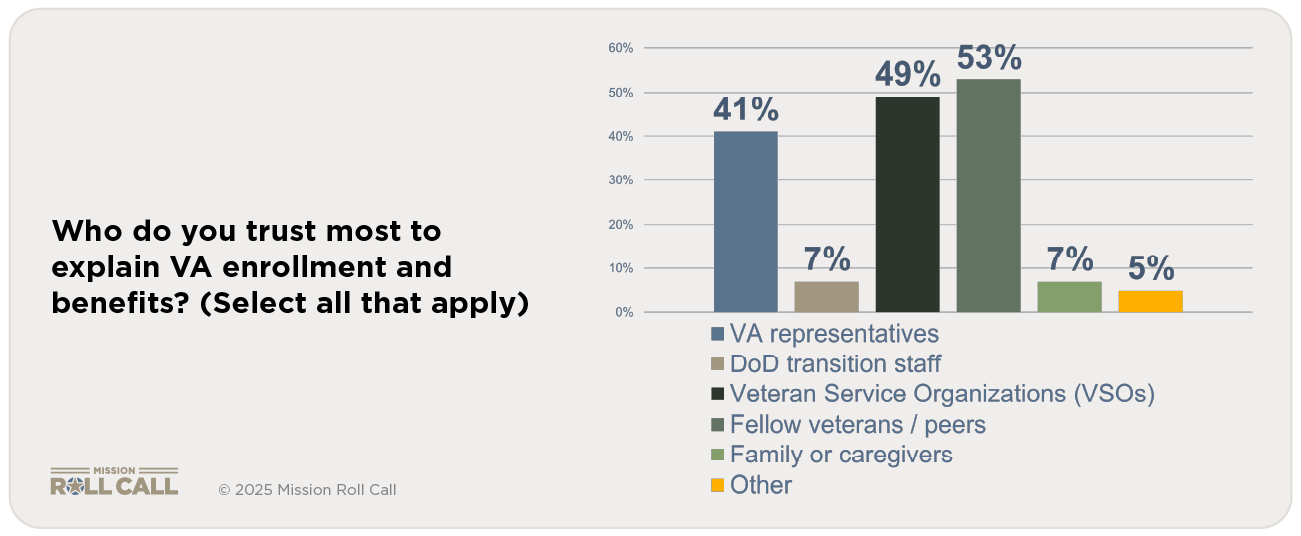
This reliance on informal networks reflects a deeper breakdown in institutional trust. Veterans described receiving different answers depending on who they contacted, leading many to stop seeking official guidance altogether. As one veteran put it, “Every office gave me a different answer, so I just listened to people who had already been through it.” As a result, veterans often navigate one of the most complex transitions of their lives through word of mouth rather than through clear, reliable, and accountable support systems.
Fuel Veteran Voices
A small gift powers the research and advocacy that brings veterans to the decision-making table.
Donate $5+